Vaccine profiles: Rotavirus
Before vaccines became available, almost every child had been infected with rotavirus by their fifth birthday, and it claimed half a million lives each year.
- 30 March 2023
- 7 min read
- by Linda Geddes

In the 1970s, several research groups set out to find out how many children died each year from diarrhoea-related illness. While their initial estimates were imprecise – ranging from three million to 12 million deaths per year – their scale focused medical and public health attention on the deadly impact that diarrhoea has on child survival.
Back then, a causative agent could be identified in fewer than 15% of diarrhoeal episodes. These included the bacteria that cause cholera and salmonella, several parasites and various environmental toxins.
Globally, rotaviruses are the leading cause of severe diarrhoea in young children. Before vaccines became available, almost every child had been infected by their fifth birthday and rotaviruses caused an estimated 500,000 deaths each year.
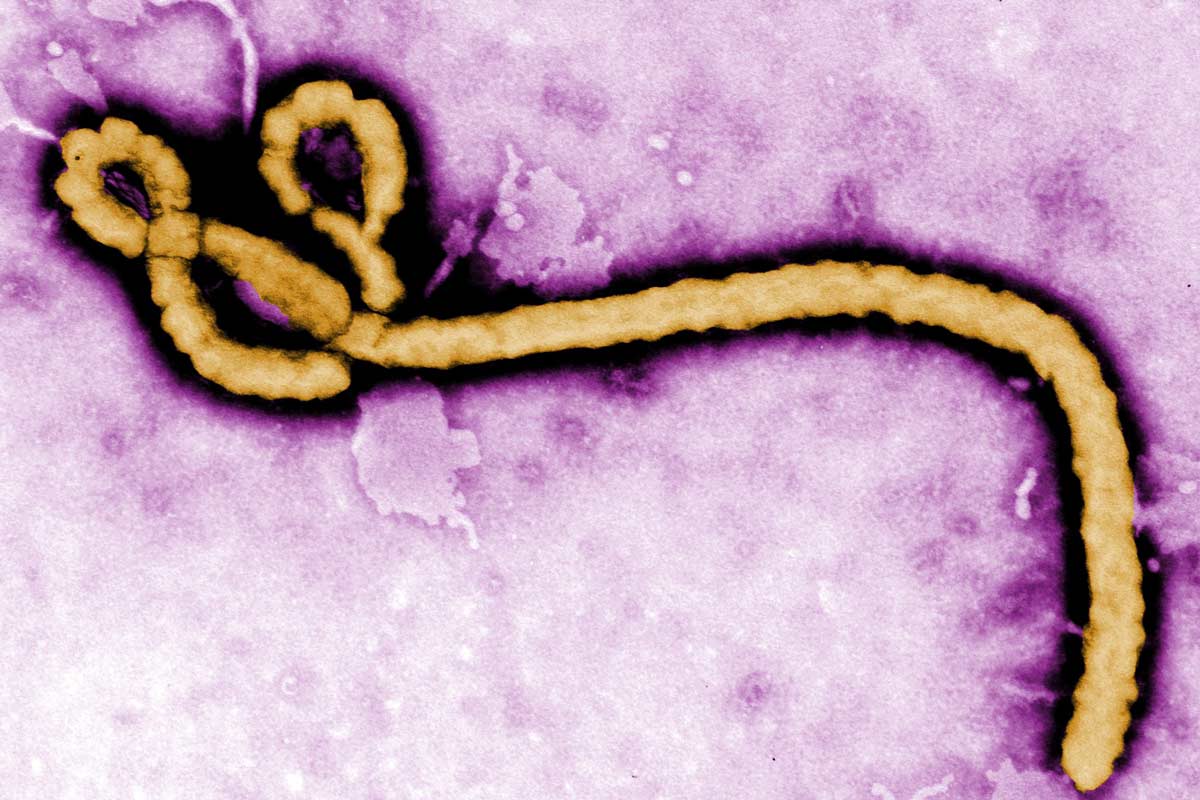
But advances in electron microscopy soon began to open a window on the plethora of other pathogens infecting children's guts and making them unwell. One of them was a beautiful but deadly wheel-shaped virus isolated from the small intestines of children with gastroenteritis. It was named rotavirus.
We now know that, globally, rotaviruses are the leading cause of severe diarrhoea in young children. Before vaccines became available, almost every child had been infected by their fifth birthday, and rotaviruses caused an estimated 500,000 deaths and two million hospitalisations worldwide each year.
Routine immunisation has greatly reduced this toll in those countries that have introduced it, but the current generation of vaccines doesn't provide full protection against infection. Thankfully, work is already underway to develop the next generation of vaccines that could prevent many more diarrhoeal deaths.
Diarrhoeal disease
Rotavirus is an RNA virus that is shed in the stool (poo) of infected people. It is mainly passed to others through contact with unwashed hands, contaminated surfaces or objects, or eating food prepared by someone who hasn't properly washed their hands.
Symptoms typically start one to three days after infection, with fever and vomiting followed by watery diarrhoea. These symptoms usually resolve within a week, but can last for as long as three weeks.
There is no specific treatment, apart from oral rehydration therapy (which involves drinking a beverage containing water, sugar, and electrolytes), rest and taking drugs to reduce fever. In roughly one in 50 cases, children develop severe dehydration, which usually requires them to be hospitalised and given fluids through a nasal tube or intravenous drip. If this treatment is delayed, it can result in death.
Infections tend to follow a seasonal pattern in countries with temperate climates, peaking in the winter and spring.
Rotavirus was first discovered in 1973 by an Australian team led by Ruth Bishop, a bacteriologist at the University of Melbourne. Seeking to identify the cause of childhood gastroenteritis, they sent intestinal biopsies from infected children to be examined under an electron-microscope. This revealed that the cells were infected with a striking-looking wheel-shaped virus.
Subsequent studies confirmed that this virus was the cause of the severe diarrhoeal illness that was claiming so many children's lives – but also that once children had been infected, they were protected against future severe rotavirus illness. This discovery sparked hope that rotavirus could be prevented through vaccination.
Rotavirus vaccines
In 1983, the first rotavirus vaccine candidate entered clinical trials in human infants. Derived from a rotavirus strain that infects cattle, it proved to be safe and capable of stimulating an immune response that provided significant protection against severe disease in some, but not all, infants.
Further vaccine candidates followed, developed from human and monkey strains of rotaviruses. The first to be licensed was RotaShield, an oral vaccine containing a mixture of live monkey and human rotaviruses that had been treated to prevent them from causing disease. It was licensed for use in the US in 1998, but withdrawn a year later after surveillance identified a small increase in the risk of intussusception, a rare type of bowel obstruction, in the week after infants received their first dose.
The trials were enormous, involving more than 60,000 infants, and demonstrated that these vaccines were both safe and effective, protecting against severe disease or hospitalisation with an efficacy of 85% to 95%.
Because of this setback, the manufacturers of two other live oral rotavirus vaccine candidates were compelled to conduct large clinical trials to investigate whether their candidates were safer. The trials were enormous, involving more than 60,000 infants, and demonstrated that these vaccines were both safe and effective, protecting against severe disease or hospitalisation with an efficacy of 85% to 95%.
In 2006, these vaccines, known as Rotarix and RotaTeq, were licensed for use in Europe and/or the US and Canada. Both are oral vaccines containing live viral particles that have been weakened, meaning they still trigger an immune response but cannot cause disease. Rotarix (GlaxoSmithKline) contains one rotavirus strain, and RotaTeq (Merck) five.
Routine immunisation
In 2009, The World Health Organization (WHO) recommended that rotavirus vaccination be included in all national immunisation programmes, following the release of data that evaluated vaccine efficacy in countries with high rates of child deaths from rotavirus disease.
Since then, two further oral vaccines have received WHO prequalification, allowing their procurement by UNICEF and Gavi for use in low-income countries: Rotavac (Bharat Biotech) and Rotasil (Serum Institute).
All these vaccines are recommended for use in infants, starting from six weeks of age. Rotarix is given as two vaccine doses, four weeks apart, while RotaTeq, Rotavac and Rotasil are given as three doses, four weeks apart.
The efficacy of these vaccines appears to vary between countries. They are most effective in countries with the lowest rates of rotavirus-associated death, and least effective in countries with the highest rates. Scientists are still trying to understand why, but malnutrition and stunting appear to play a role, and recent studies have suggested that intestinal inflammation linked to poor sanitation and hygiene, and differences in the composition of the gut microbiome may also be implicated.
Have you read?
According to a recent Cochrane Review, which assessed the efficacy of all four WHO prequalified vaccines, rotavirus vaccines prevent more than 90% of severe cases of rotavirus diarrhoea in countries with low child mortality rates, more than 75% in countries with medium child mortality rates, and 35% to 58% in countries with high child mortality rates.
However, because countries that have high child mortality rates have far more severe rotavirus cases and deaths in the absence of vaccination than countries with low child mortality rates, rotavirus vaccines prevent far more suffering in countries with high child mortality rates, despite their lower effectiveness in these countries.
Substantial impact
So far, more than 100 countries have introduced rotavirus vaccines into their routine immunisation programs. The impact of this has been substantial. An analysis of data from 69 countries participating in the WHO's Global Rotavirus Surveillance Network (GRSN) found a 40% reduction in the prevalence of rotavirus among children admitted to hospital with severe gastroenteritis, following vaccine introductions.
A separate review of data from 49 countries that have introduced routine rotavirus vaccination reported a roughly 59% reduction in hospitalisations for gastroenteritis, and a 36% reduction in deaths from gastroenteritis among children aged under five years.
Rotavirus vaccination also appears to have delayed the onset and decreased the magnitude of the rotavirus season in some countries.
Future vaccines
Although live oral rotavirus vaccines have succeeded in reducing severe diarrhoea everywhere they've been introduced, they would prevent even more cases and deaths if they were more effective, especially in the countries with the highest child mortality rates.
The cost of these vaccines has also hindered their uptake in some countries, particularly countries with low child mortality rates, although Gavi has supported their rollout in 52 low and middle-income countries, which means now more countries in Africa are using rotavirus vaccines than in Europe. However, various next-generation rotavirus vaccines are currently in development that may be even better than current ones.
Rotavirus vaccine and improved sanitation have dramatically reduced the toll from diarrhoeal illness in recent decades, but too many children still die from the dehydration it causes. The next-generation of rotavirus vaccines may address key barriers to their uptake, and further reduce this toll.
Injectable vaccines, such as the trivalent P2-VP8 candidate currently being evaluated in Ghana, Malawi, and Zambia, are expected to perform better than oral vaccines in countries with a high burden of rotavirus disease because they bypass the gut, which scientists think could account for the observed differences in efficacy.
Such vaccines would be relatively easy to introduce into existing routine childhood immunisation schedules, because they could be given alongside other injectable vaccines. Alternatively, they could be combined into existing shots, such as the DTP-pentavalent vaccine (which prevents five diseases – diphtheria, tetanus, pertussis, Haemophilus influenzae type B and hepatitis B). This could make it easier to deliver protection against rotavirus, at a lower cost.
Next-generation oral vaccines, designed to be taken at birth and followed by two further infant doses, are also being tested, with preliminary evidence suggesting that one such candidate may be more effective than existing vaccines.
Rotavirus vaccine and improved sanitation have dramatically reduced the toll from diarrhoeal illness in recent decades, but too many children still die from the dehydration it causes. The next-generation of rotavirus vaccines may address key barriers to their uptake, and further reduce this toll.