How women’s cooperatives in India emerged as COVID-19 first responders
Integrating COVID-19 campaigns into the work that the Self-Employed Women’s Association does ensured that rural communities were not left out.
- 5 October 2022
- 5 min read
- by Ananta Seth

India’s civil society organisations (CSOs) emerged as first responders during the pandemic. Due to limited state healthcare capacity and infrastructure, these organisations played a pivotal role in delivering necessities such as rations and health supplies to the most vulnerable and hard-to-reach citizens.
They also led community mobilisation and awareness campaigns to promote preventative measures such as vaccinations, social distancing and mask-wearing.
The government has acknowledged the importance of over 92,000 registered CSOs for their contribution to the COVID-19 response. Women’s groups and cooperatives, drawing from decades of community-based experience, were uniquely positioned to deliver health information. The Self-Employed Women’s Association (SEWA), India’s largest union of informal women workers, was at the forefront of the COVID-19 response from the beginning of the pandemic.
These are women who have cultivated strong, trusting relationships with their communities over the years. Along with strong messaging from the government, their credibility was an important factor in ensuring that people accessed vaccine services.
SEWA has over 15 years of experience in providing comprehensive primary health care to informal workers with a multi-pronged approach that focuses on health information and awareness, referrals, livelihoods and social security, including healthcare, childcare, insurance, pension and housing.
The union, with a membership of two million informal workers, has the reach, network and expertise to raise health awareness and carry out vaccine advocacy activities in more than 18 states across the country. In many low-income areas, SEWA’s community health workers were, therefore, the first line of defence to combat the pandemic.
Supported by the WHO and India’s Ministry of Health and Family Welfare, SEWA developed an evidence-based community engagement framework for dissemination of accurate information on COVID-19 and vaccines, leveraging SEWA’s existing organised base of informal women workers.
Have you read?
Susan Thomas, National Health Coordinator, says: “We were able to leverage technology and social media to mobilise our base of women leaders within the first few weeks of the pandemic.
“We used these platforms to disseminate trusted sources of information, as misinformation was rife, especially in the earlier stages of the pandemic. These messages were made attractive, reader-friendly and as concise as possible, while including all relevant information.
“Moreover, as our members and their families could not access health services during the government mandated lockdown, we developed a platform for medical tele-consultation services and our community health workers delivered medicines to these families. In collaboration with the government, we also mapped out areas with low vaccination rates and reached out to the community members to promote uptake of vaccines.”
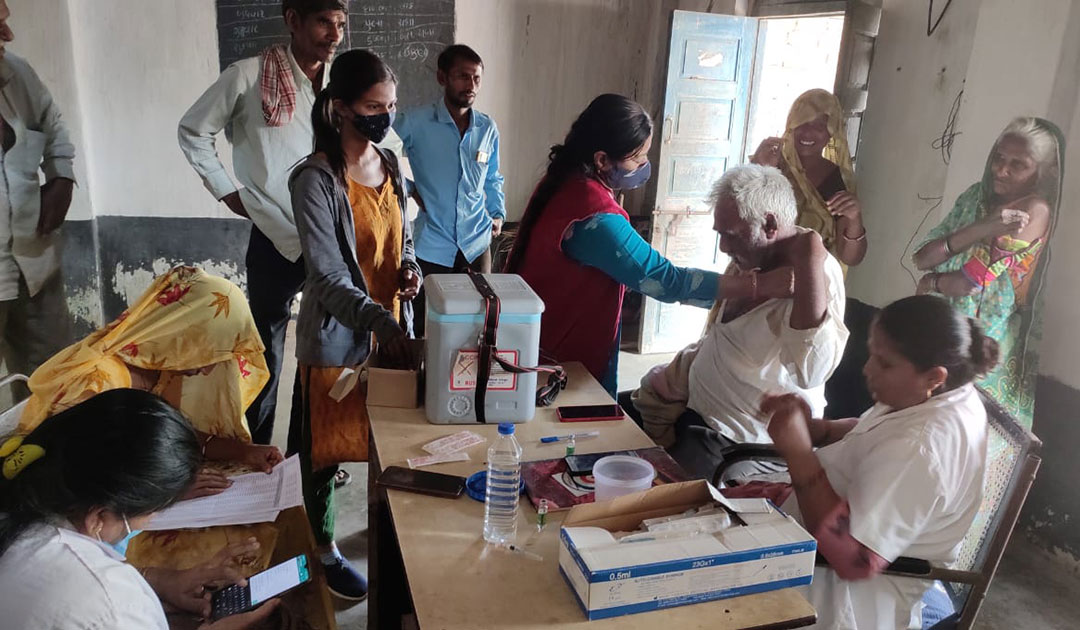
Drawing from SEWA’s efforts in Gujarat, Yasmin Sheikh, Health Coordinator for the state, says: “Under the COVID-19 Rakshak (Protect against COVID-19) programme, SEWA carried out surveys on household vaccine status in areas with a low take-up of vaccines. During these surveys, community health workers also addressed any fears and concerns about the vaccines using leaflets and short videos in the local language.
“The survey results were shared with primary healthcare centres and informed the government’s decision to organise vaccine camps in areas that were falling behind. This was particularly effective in getting rural communities vaccinated as they did not have to travel long distances to visit the nearest health centre. We worked closely with the government to get the vaccines to these communities.”
Susan Thomas continues: “SEWA has the advantage of a strong community presence. We were not mobilising external stakeholders but building the capacity of a cadre of women leaders belonging to these communities.
“These are women who have cultivated strong, trusting relationships with their communities over the years. Along with strong messaging from the government, their credibility was an important factor in ensuring that people accessed vaccine services.
“They were among the first to receive the vaccines, which led to more positive community perceptions of the vaccine. We were also providing additional support services such as referral for prenatal and antenatal care, other sexual and reproductive health services, and reminders for childhood routine immunisation.”
Mirai Chatterjee, Director of SEWA Social Security, underlines how the unions’ integrated approach played a significant role in building trust among community members.
Chatterjee says, “Trust is central to how SEWA operates. From social protection to livelihood support, our community-based leaders and health workers have served their people in times of hardship. Our approach of collective organising and linkages with government health services contribute to the success of our community-based approach.”
An effective response to COVID-19 and future pandemics requires coordination across multiple sectors, guided by strong leadership at all levels of the health system. This includes organisations like SEWA that work at the grassroots, often with the most marginalised communities.
The SEWA experience in India underscores the importance of union cooperatives, especially in informal worker communities with a lack of access to health services. Importantly, it is a reminder that female community health workers serve as a bridge between the health system and the community. Since they come from the communities they serve, they are often the best placed to understand, and work within, cultural and gender norms and power dynamics.
More from Ananta Seth






