Is the COVAX Facility ensuring equitable vaccine distribution?
A new study has looked into how effective COVAX has been in its central aim: reducing the disparity between rich and poor when it comes to access to COVID-19 vaccines.
- 29 March 2022
- 3 min read
- by Joshua Mak , Akriti Mehta , Katelyn Jison Yoo , Bryan Patenaude

The COVID-19 Vaccines Global Access (COVAX) Facility was created under the premise that effective control of the pandemic will require equitable allocation and distribution of COVID-19 vaccines worldwide. During the COVID-19 global response, concerns of vaccine nationalism, i.e., wealthier nations with substantial market power receiving a larger, disproportionate share of COVID-19 vaccines given their population, were prevalent. The COVAX Facility aimed to address this disparity by consolidating the vaccine demand of lower-income nations to bargain with pharmaceutical manufacturers directly.
The COVAX Facility global risk-sharing mechanism of pooled vaccine procurement has made significant strides toward achieving its goal of distributional equity among the world’s most disadvantaged economies.
Now that the COVAX Facility has been established for almost two years, we ask: has the COVAX Facility been effective in fulfilling its purpose?
Researchers from the World Bank and the Johns Hopkins Bloomberg School of Public Health’s International Vaccine Access Center (IVAC) collaborated on a study to assess how the benefits of COVID-19 vaccine doses were distributed among COVAX-participating countries as of early-January 2022. These include countries with lower GDP per capita values that qualified for financial support under the COVAX Advance Market Commitment (AMC) and those that self-financed the vaccine doses.
Have you read?
Disparities in COVID-19 vaccine doses allocated and doses delivered
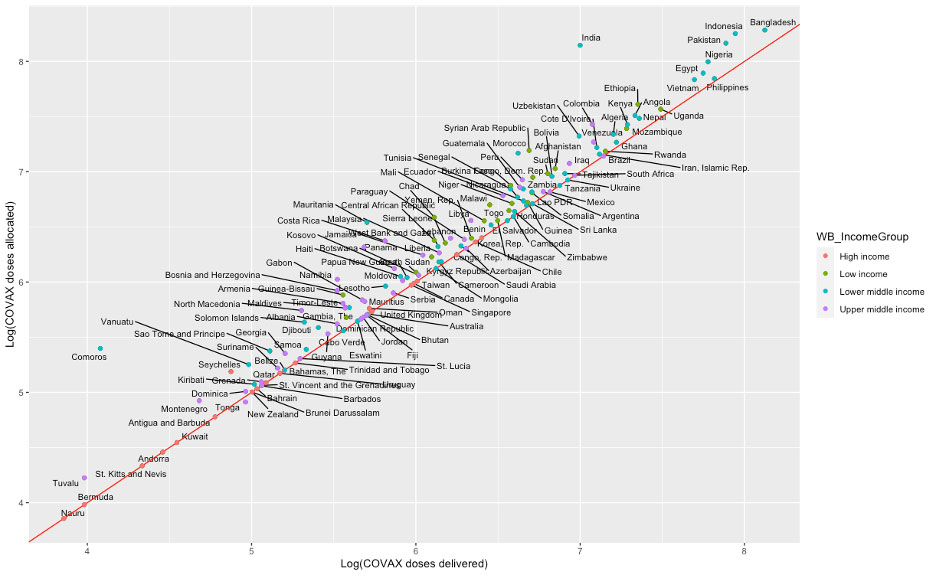
The analysis differentiates between doses allocated to each country and doses actually delivered to the countries. Though some countries received the full number of doses allocated, others await the remaining difference.
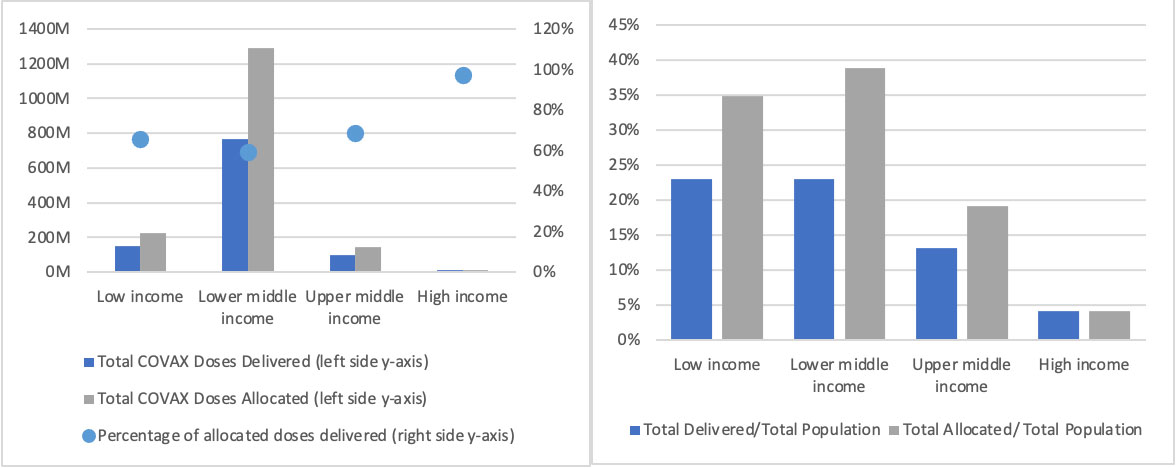
The bulk of allocated and delivered COVAX vaccine doses are designated for low and lower-middle income countries. After adjusting for allocated and delivered doses as a proportion of total population, it is shown that low-income and lower-middle income countries experience the greatest proportional gaps between allocated and delivered vaccine doses.
Assessing dose delivery equity between AMC and self-financing COVAX participants
Distribution of COVAX Facility vaccine benefits was assessed with a benefit incidence analysis. Cumulative vaccine benefits were measured against cumulative countries ranked by their 2019 GDP per capita purchasing power parity. Resulting concentration curves are compared against the 45-degree line of perfect equality.
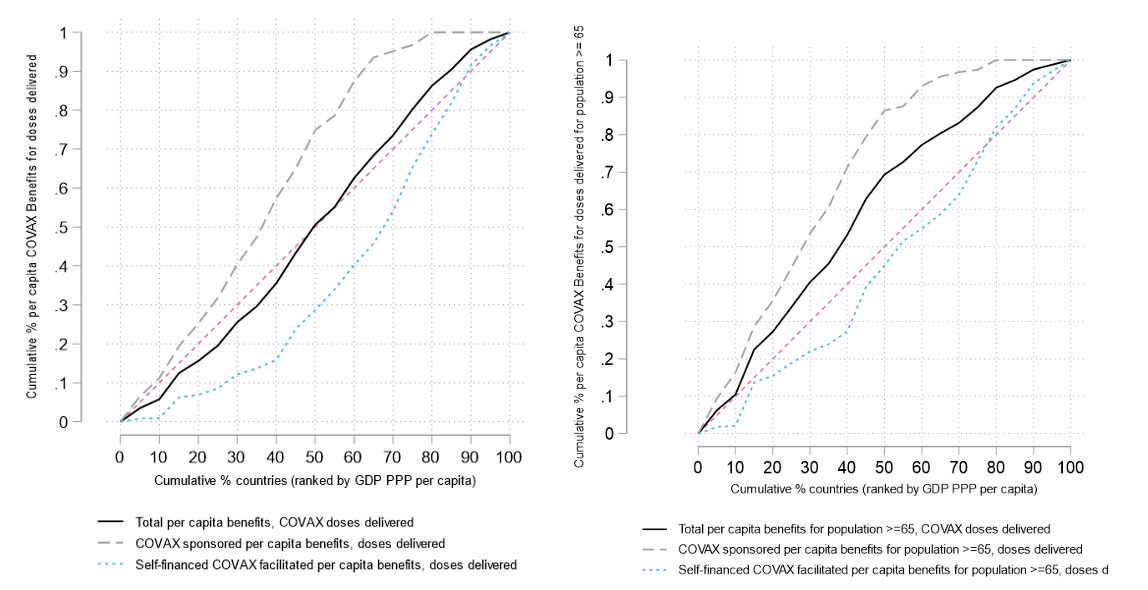
For both scenarios looking across the entire population and the high-need population (proxied by number of adults aged 65 years and older), wealthier self-financed countries and territories experience a greater portion of benefits compared to their poorer counterparts as seen in the concentration curves lying below the line of equality. They may be a function of wealthier players having more resources to procure additional doses beyond those secured by COVAX.
However, among countries and territories qualifying for AMC support, poorer ones experienced greater benefits than wealthier ones for both population scenarios. This is evidence that the COVAX Facility global risk-sharing mechanism of pooled vaccine procurement has made significant strides toward achieving its goal of distributional equity among the world’s most disadvantaged economies.
What does this mean?
Success of the COVAX Facility in achieving equitable distribution of COVID-19 vaccines is an example of how systems of bundled procurement and risk-sharing can improve access for countries and territories with low individual market visibility. Expansion of COVAX benefits among participants can help decrease the disparities in accessibility that exists between lower and higher income economies during pandemic situations.
Authors
- Joshua Mak
- Katelyn Jison Yoo
- Akriti Mehta
- Bryan Patenaude
More from Joshua Mak





